
Content
Module 4: Medications - Advanced Knowledge
Airway anatomy
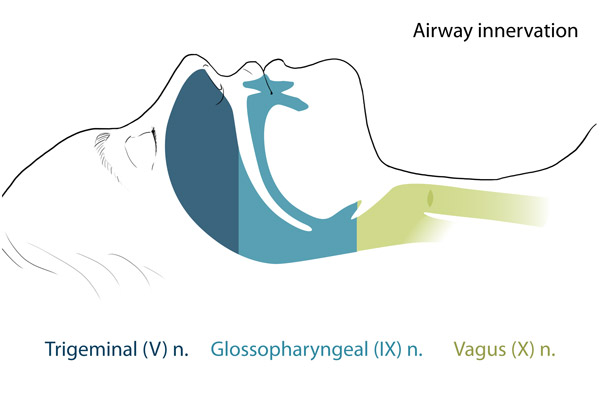
nerves or their branches can selectively be blocked for an awake bronchoscopic intubation:
- Trigeminal nerve (CN V) (nasal cavity, mouth)
The nasal cavity is entirely innervated by the trigeminal nerve.
- Anterior ethmoidal nerve (from V1) – septum
- Greater and lesser palatine nerves, from sphenopalatine ganglion in pterygopalatine fossa (V2)
- Nasopalatine nerve, from sphenopalatine ganglion (V2) – septum
- Glossopharyngeal nerve (CN IX) (posterior 1/3 tongue, pharynx, valleculae, lingual surface of epiglottis and gag reflex)
Gag reflex:
- Elicited by stimulation of the glossopharyngeal nerve, efferent from vagus nerve
- Abolished by bilateral block of glossopharyngeal nerve
- Vagus nerve (X) (larynx, trachea)
The superior laryngeal nerve divides into internal and external branches.
- Internal branch: sensation from epiglottis to above vocal cords
- External branch: cricothyroid muscle
Recurrent laryngeal nerve:
- Given off the vagus nerve during it's intra-thoracic course (loops around ligamentum arteriosum on left and around subclavian artery on right)
- Provides sensation of larynx below and including vocal cords and trachea. Motor to all intrinsic muscles of the larynx except cricothyroid muscle
- Glottic closure reflex (exaggeration of this reflex = laryngospasm) – this is caused by stimulation of superior laryngeal nerve, efferent from recurrent laryngeal nerve
Nerve blocks
Superior laryngeal nerve (sensation to larynx above vocal cords)
- Blocked between hyoid bone and thyroid cartilage where it penetrates the thyrohyoid membrane
- Place patient supine with maximal neck extension
- Grab the hyoid between the thumb and index finger and firmly displace it towards the side to be blocked
- Advance a 25g needle to the greater cornu then walk it off inferiorly and advance it a further 2 – 3mm
- Inject 2 – 3ml and an additional 1ml as the needle is withdrawn (to block the external branch)
Glossopharyngeal nerve: (gag reflex and sensation from the oropharynx to the lingual surface of the epiglottis)
- Usually blocked by the local anesthetic applied to the back of the tongue and throat
- Can also be blocked by holding a local anesthetic soaked swab bilaterally at the palato-glossal arch (the rim of tissue than runs from the uvula to the base of the tongue)
_sm.jpg)
The glossopharyngeal nerve can be blocked by holding swabs soaked in local anesthetic at the point indicated by the white arrow.
Continue to: Module 5: Procedure
