Please enable JavaScript to use all features of this page.
Synopsis of Calcific Aortic Stenosis
Acknowledgements
- Dr. I. Smith Cardiac anesthesia fellow*
- Dr. M. Wasowicz Staff anesthetist*
- Dr. A. Jerath Staff anesthetist*
- Dr. A. Vegas Staff anesthetist*
- Dr. C. Feindel Staff surgeon†
| * | Department of Anesthesia and Pain Management, Toronto General Hospital |
| † | Department of Surgery, Toronto General Hospital |
Synopsis
Definition
- Calcific Aortic Stenosis Calcification of the AV cusps leading to a narrowed valve orifice with antegrade flow restriction and turbulence
- Aortic sclerosis Valve thickening without obstruction to LV outflow tract1
Gender and Prevalence
- Calcific Aortic Stenosis M > F, 2% > 65 years, 4% > 85 years2,3
- Aortic Sclerosis M > F, 26% > 65 years, 48% > 85 years4
Etiology
- Congenital Rare, although may be associated with uni- or bicuspid AV
- Acquired Majority of cases. Risk factors include male gender, smoking, hyperlipidaemia and metabolic syndrome5
Pathophysiology
- AS and sclerosis involves a local athero-inflammatory process similar to atherosclerotic disease
- Calcification involves the base and body of the cusp without commissural fusion1, 6
- Flow restriction and systolic pressure overload leads to compensatory increase in LV wall thickness in order to maintain SV and minimize LV systolic wall stress. This leads to diastolic dysfunction and reduced coronary vasodilator reserve with the myocardium at risk of subendocardial ischemia, fig. 1, 2, 3a & 3b.
- Females demonstrate greater LV wall thickening and cavity obliteration than males
- Low-flow Low-gradient AS occurs with LV systolic dysfunction and severe AS
- Defined by EOA < 1 cm2, LV EF < 40%, mean pressure gradient < 30-40 mmHg6, 7
- Results from either inadequate LVH in response to the high afterload or poor contractile state, for example CAD
- Sclerosis May progress to valve calcification with valvular outflow obstruction. Associated with increased cardiovascular mortality4
Clinical Presentation
- Symptom onset Commonly at 70-90 years of age
- Early symptoms Reduced exercise tolerance from diastolic dysfunction
- Late symptoms Angina (35%), syncope (15%), heart failure (50%)8
Imaging & Investigations
- ECG LV strain, LVH, LBBB
- CXR Aortic root calcification and post-stenotic aortic dilatation
- Echocardiography Assess AV morphology, function, associated features and grade severity, see echo features table. The following are used to grade severity with various caveats6
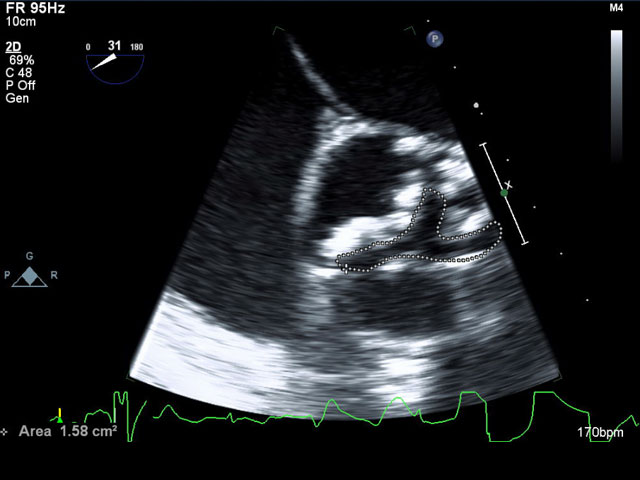
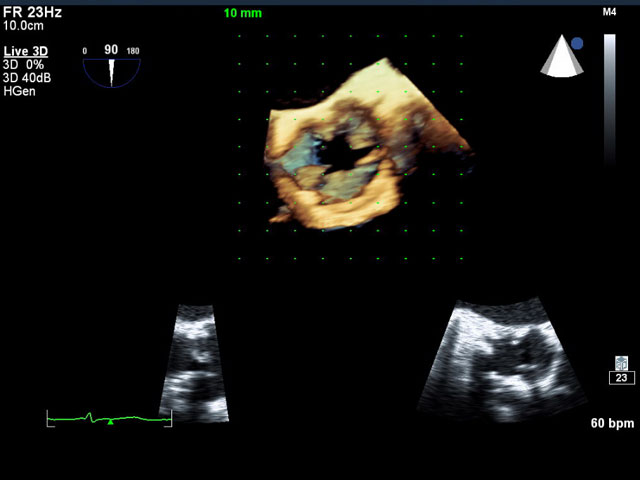
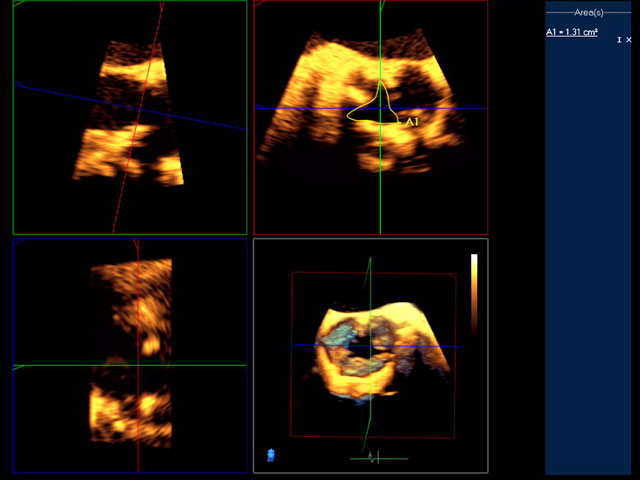
- AV planimetry Rapid estimation of anatomical AVA, though often overestimates. Technically difficult due to poor cusp definition from heavy calcium deposition, acoustic shadowing and reverberation artifact9, fig. 4, 5a and 5b.
- AS jet velocity Requires parallel alignment of CW Doppler through the narrow orifice to avoid underestimating velocity. If the rhythm is irregular average at least 3 readings. Measurements are flow dependent, i.e low cardiac output states will produce lower transvalvular velocities and lead to underestimation of severity
- Mean aortic pressure The maximum transvalvular pressure gradient is calculated using the peak jet velocity and the Bernoulli equation, Pmax = 4Vmax2 Mean gradient is measured by tracing the CW spectral Doppler which averages the instantaneous gradient over time. The mean gradient can also be estimated from the peak velocity,Pmean = 2.4Vmax2Use the modified Bernoulli equation if the VLVOT exceeds 1.5 m/sec,P = 4(VAV2 –VLVOT2)As jet velocities are used to calculate pressure gradients, these measurements are similarly flow dependent, fig. 6a and 6b.
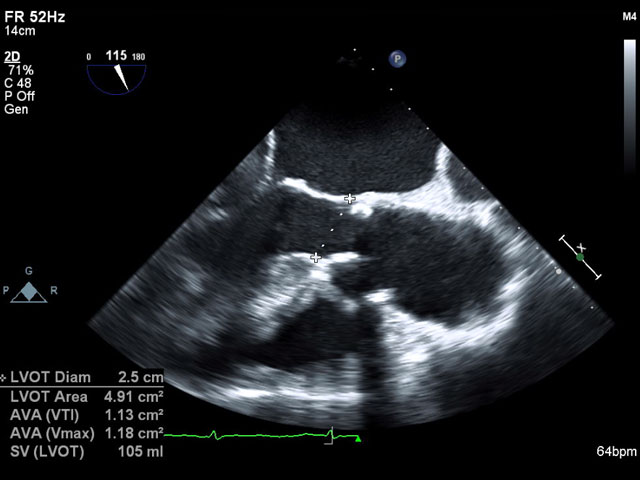
- Valve area Continuity equation forms the most reliable technique to measure the effective or physiologic AV area, AVA = CSALVOT x VTILVOT / VTIAV The effective AVA is smaller then the anatomic AVA due to flow stream retraction at the orifice. Greatest source of error arises within the squared measurement of LVOT diameter. Pressure recovery occurs in a small aorta and overestimates AVA, fig 6
- Dimensionless velocity index This is the ratio of either the velocity or VTI of the LVOT over the AV, V (VTI)LVOT / V (VTI)AV Values below 0.25 indicate severe stenosis. DVI is flow independent, ie values are unaffected by changes in cardiac output, fig. 6a and 6b.
- Dobutamine stress echocardiography assesses contractile reserve, peak VAS, mean gradient, EF in low-flow low-gradient AS. Patients displaying no contractile reserve with SV and EF rising < 20% have a higher surgical mortality6
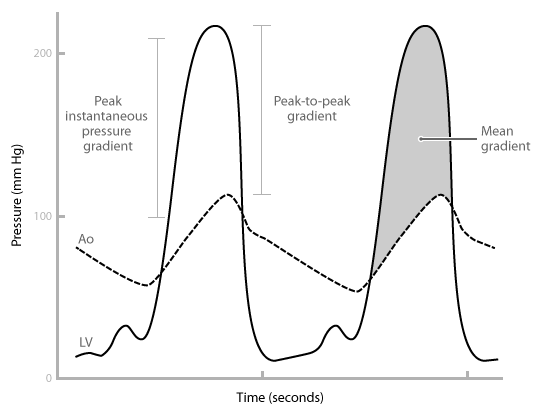
- Cardiac catheterization Not recommended to grade AS severity unless echo inconclusive. Cardiac cath measures the peak to peak gradient between the LV and aortic pressure. This underestimates the severity as it is lower than the peak instantaneous pressure gradient which is measured by echocardiography, fig. 8. AVA can be determined using the Gorlin formula, AVA = CO / 44.3 x SEP x HR x √PmeanAccurate estimation of AVA is affected by arrhythmias and is flow dependent, ie high cardiac output states may overestimate valve area. Catheterization aids in the identification of concomitant CAD1
- Classification of AS Severity
| Severity |
V (m/sec) |
Mean gradient (mm Hg) |
AVA (cm2) | IVA | VR |
|---|
| Mild |
2.6-2.9 | < 20 | > 1.5 | > 0.85 | > 0.5 |
| Moderate | 3-4 | 20-40 | 1-1.5 | 0.6-0.85 | 0.25-0.50 |
| Severe | > 4 | > 40 | < 1 | < 0.6 | < 0.25 |
- Typical progression of AS Increase jet velocity 0.3 m/sec/year, increase mean pressure gradient 7mmHg/year + decrease AVA 0.1cm2/year1, 12
Indicators for Surgical Intervention
- Medical therapy Limited role. Statins may slow disease progression. Management of hypertension, AF and digoxin for LV systolic dysfunction 3, 11
- Surgical Intervention Treatment of choice. Operative indications1:-
- Symptomatic Isolated severe AS or combined with CABG, aortic or other valvular surgery1
- Asymptomatic patients Controversial. Consider operative intervention in severe or mild-moderate AS if there is high risk of rapid progression (age > 50 years, heavily calcified valve and CAD) or patients develop symptoms or hypotension during exercise1, 10, 11
- Mild-moderate AS patients undergoing CABG and likely rapid progression
- LV dysfunction LV function can improve after AVR in severe AS with low EF. LV contractile dysfunction not caused by afterload mismatch is associated with greater overall mortality but may improve survival despite incomplete symptom resolution
Surgical Options
- Balloon valvuloplasty Performed only as a palliative procedure in non-operative candidates or bridge to surgery in hemodynamically unstable patient due to high re-stenosis rate
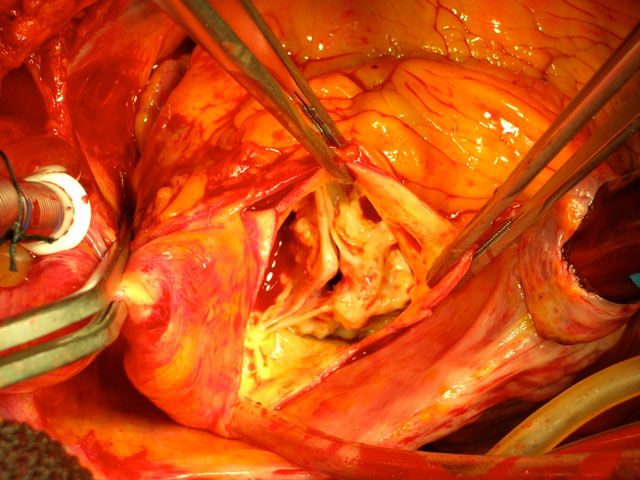
- Open valve replacement Mechanical or bioprosthetic valve placed using CPB, fig. 9.
- Percutaneous valve replacement Retrograde transfemoral/subclavian or antegrade transapical bioprosthetic AVR can be performed without the use of CPB in elderly poor operative candidates13-18, fig. 7a, 7b, 7c, 7d, 7e, 7f, 7g, 7h, 7i, 7j,7k, and 7l.
Complications
- Myocardial Ischemia
- Infective endocarditis
- LV diastolic and systolic dysfunction
- Arrhythmias
- Impaired platelet function and acquired VWF deficiency1
Survival
- No surgical intervention Mortality from the onset of angina, syncope and CHF are 5, 3 and 2 years respectively3
- Operative mortality Open AVR 3% rising to 14% with advanced age, co-morbidities and combination cardiac procedures19
- Mechanical valves Good long term survival with 5 year event-free survival from thromboembolic and hemorrhagic complications 98-99%20. Requires oral anticoagulation
- Bioprosthetic valves No long-term anticoagulation required. Shorter valve lifespan with 25% requiring redo surgery at 10 years
- Complications post AVR Paravalvular leaks, infective endocarditits, hemorrhagic complications associated with oral anticoagulation
- Patient prosthesis mismatch Residual stenosis and persistent symptoms of CHF from insertion of a valve with indexed EOA less than 0.85 cm2/m2. PPM associated with higher early and late overall mortality.21,24 Prevention is by insertion of an appropriately sized prosthesis with indexed EOA greater than 0.85 cm2/m2 which may require aortic root enlargement or use of a larger area stentless valve
- Percutaneous AVR 30 day mortality 6.3 - 12.3%16-18, 27
- Complications of transfemoral or transapical AVR Device embolization, paravalvular leak, mitral regurgitation, myocardial ischemia from coronary occlusion, tamponade, aortic root rupture.
Echo Features
TEE views used for diagnosis
- ME AV SAX
- ME AV LAX
- TG mid SAX
- TG LAX
- Deep TG
What to look for in 2D and 3D TEE
- Cusp number (uni-,bi-,tri-,quadra-cuspid)
- Assess for valve calcification + reduced valve orifice
- Reduced cusp excursion valve
- AV planimetry9
- Aortic root dimensions
- Post-stenotic aortic dilatation
- Identify additional calcium deposits on the mitral annulus (MAC) + aorta
What to look for in Colour Doppler
- Identify flow turbulence distal to AV
- Assess severity + location AI
What to look for in Spectral Doppler
- PW Doppler LVOT to assess peak/mean pressure gradients+ VTILVOT (continuity equation)
- PW Doppler LVOT dagger shaped waveform if septal hypertrophy
- CW Doppler AV to assess peak/mean pressure gradients + VTIAV
- AI PHT/Deceleration time
Differential Diagnosis
Prosthetic valve stenosis
- Degeneration and pannus formation or endocarditis of an old prosthetic
- Patient prosthetic valve mismatch can lead to obstructive symptoms when an inappropriately small sized valve is implanted
Rheumatic aortic stenosis
- Fusion of commissures reduce systolic cusp excursion and create a narrowed + circular orifice
Uni-, bi-, quadricuspid aortic valve disease
- Calcification of a non-trileaflet valve can lead to valvular stenosis + regurgitation
- Diastole may reveal altered cusp number + morphology but presence of a raphe within a bicuspid valve can often be mistaken for a tri-leaflet valve
- Systole often reveals eccentric cusp opening + altered cusp number
Endocarditis
- Formation of vegetations often occur on a pathological native or prosthetic AV with reduced systolic surface area
- Masses are usually mobile + located on the LV side of the AV
- Associated complications include aortic root abscess, fistulae formation + pseudoaneurysm
Associated Conditions
LV function and Mitral valve disease
Views
- ME 4C
- ME 2C
- ME LAX
- TG SAX
2D/3D
Colour Doppler
Spectral Doppler
Post aortic valve replacement
Views
- ME AV SAX
- ME AV LAX
- TG LAX
- Deep TG
2D/3D
Colour Doppler
Spectral Doppler
References
- Bonow R et al. 2008. Focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association task force on practice guidelines. J Am Coll Cardiol 2008; 52: e1-142.
- Stewart BF et al. 1997. Clinical factors associated with calcific aortic valve disease. J Am Coll Cardiol; 29: 630-4.
- Carabello B, Paulus W. 2009. Aortic Stenosis. Lancet; 373: 956-66.
- Otto CM et al. 1999. Association of aortic-valve sclerosis with cardiovascular mortality and morbidity in the elderly. N Eng J Med; 341: 147-57.
- Parolari A et al. 2009. Non-rheumatic calcific aortic stenosis: an overview from basic science to pharmacological prevention. Eur J Cardiothorac Surg; 35: 493-504.
- Baumgartner H et al. 2009. Echocardiographic assessment of valve stenosis: EAE/ASE recommendations for clinical practice. Eur J Echo; 10: 1-25.
- Burwash I. 2007. Low-flow, low gradient aortic stenosis: from evaluation to treatment. Curr Opin Cardiol; 22: 84-91.
- Ross J Jr, Braunwald E. 1968. Aortic stenosis. Circulation 1968; 38: 61-7.
- Gilon D et al.2002. Effect of three-dimensional valve shape on the hemodynamics of aortic stenosis: three-dimensional echocardiographic stereolithography and patient studies. J Am Coll Cardiol; 40: 1479–86.
- Rosenhek R et al.2004. Mild and moderate aortic stenosis.Natural history and risk stratification by echocardiography. Eur Heart J; 25: 199-205.
- Rosenhek R et al. 2000. Predictors of outcome in severe asymptomatic aortic stenosis. N Engl J Med; 343: 611-17.
- Rossebø A, Pedersen T et al. 2008. Intensive lipid lowering with simvastatin and ezetimibe in aortic stenosis. N Engl J Med; 359: 1343-56.
- Rodés-Cabau J et al. 2010. Transcatheter aortic valve implantation for the treatment of severe symptomatic aortic stenosis in patients at very high or prohibitive surgical risk: acute and late outcomes of the multicenter Canadian experience. J Am Coll Cardiol; 55: 1080-90.
- Iung B et al. 2005. Decision-making in elderly patients with severe aortic stenosis: why are so many denied surgery? Eur Heart J; 26: 2714–20.
- Cribier A et al. 2002. Percutaneous transcatheter implantation of an aortic valve prosthesis for calcific aortic stenosis: first human case description.Circulation;106: 3006–8.
- Ree RM et al. 2008. Case series: anesthesia for retrograde percutaneous aortic valve replacement with the first 40 patients. Can J Anesth; 55: 761-8.
- Zahn et al. 2011. Transcatheter aortic valve implantation: first results from a multi-centre real-world registry.Eur Heart J; 32: 198-204.
- Walther T et al. 2010. Transapical aortic valve implantation in 100 consecutive patients: comparison to propensity-matched conventional aortic valve replacement. Eur Heart J;31: 1398-403.
- Jamieson WRE et al. 1999. Risk stratification for cardiac valve replacement.National Cardiac surgery datatbase. Ann Thorac Surg; 67: 943-51.
- Svensson L, et al. 2003. Surgical options in young adults with aortic valve disease. Curr Probl Cardiol; 28: 417-79.
- Pibarat P, Dumesnil J. 2006. Prosthesis-patient mismatch, clinical impact and prevention. Heart; 92: 1022-9.
- Kerut E et al. 2007. Mitral systolic anterior motion (SAM) with dynamic left ventricular outflow obstruction following aortic valve replacement. Echocardiography; 24: 658-60.
- Zoghbi WA et al. 2009. Recommendations for evaluation of prosthetic valves with echocardiography and Doppler ultrasound. J Am Soc Echo; 22: 975-1014.
- Sukernik MR et al. 2007. Systolic anterior motion of the mitral valve after aortic valve replacement for aortic insufficiency. J Cardiothorac Vasc Anesth; 21: 574-6.
- Luckie M, Khattar RS. 2008. Systolic anterior motion of the mitral valve-beyond hypertrophic cardiomyopathy. Heart; 94: 1383-5
- Wilton E et al. 2006. Post-stenotic aortic dilatation. J Cardiothorac Surg; 1: 1-11.
- Zamorano JL et al. 2011. EAE/ASE recommendations for the use of echocardiography in new transcatheter interventions for valvular heart disease. Eur Heart J; 32: 2189 – 214.
- Vahanian A et al. 2007. Guidelines on the management of valvular heart disease. Eur Heart J; 28: 230 - 68.
Abbreviations
| Abbreviation |
Term |
| AF |
atrial fibrillation |
| AI |
aortic insufficiency/regurgitation |
| AMVL |
anterior mitral valve leaflet |
| ASE |
American Society of Echocardiography |
| AS |
aortic stenosis |
| AV |
aortic valve |
| AVA |
aortic valve area |
| AVR |
aortic valve replacement |
| CAD |
coronary artery disease |
| CFD |
colour flow Doppler |
| CO |
cardiac output |
| CPB |
cardiopulmonary bypass |
| CHF |
congestive cardiac failure |
| CSA |
cross sectional area |
| CW |
continuous wave |
| CXR |
chest radiograph |
| DSE |
dobutamine stress echocardiography |
| DTG |
deep transgastric |
| DVI |
dimensionless velocity index |
| EOA |
effective orifice area |
| ECG |
electrocardiogram |
| EF |
ejection fraction |
| HR |
heart rate |
| IVA |
indexed valve area |
| LAX |
long axis |
| LBBB |
left bundle branch block |
| LV |
left ventricle |
| LVH |
left ventricular hypertrophy |
| LVOT |
left ventricular outflow tract |
| MAC |
mitral annular calcification |
| ME |
mid esophageal |
| MR |
mitral regurgitation |
| MS |
mitral stenosis |
| MVR |
mitral valve replacement/repair |
| PFO |
patent foramen ovale |
| PHT |
pressure half time |
| Pmax |
peak gradient |
| Pmean |
mean gradient |
| PPM |
prosthesis-patient mismatch |
| PVe |
pulmonary vein |
| PW |
pulsed wave |
| SAM |
systolic anterior motion |
| SAX |
short axis |
| SEP |
systolic ejection period |
| SoV |
sinus of Valsalva |
| STJ |
sino-tubular junction |
| STS |
Society of Thoracic Surgeons |
| SV |
stroke volume |
| TEE |
transesophogeal echocardiography |
| TG |
transgastric |
| V |
velocity |
| Vmax |
maximum velocity |
| VR |
velocity ratio |
| VSD |
ventricular septal defect |
| VTI |
velocity time integral |
| VWF |
Von Willebrands Factor |
Back to Top of Page

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}