
Please enable JavaScript to use all features of this page.
Synopsis of Cardiac Myxoma
Synopsis
Definition
Benign primary cardiac tumour.
Gender and Prevalence
- Female > Male
- Incidence of primary cardiac tumours 0.001 – 0.28%.
- 75% are benign tumours, of which 50% are myxomas (0.5 per million population per year).
- Any age group, higher in adults 3rd - 6th decade.
- Familial myxomas younger age in 2nd - 3rd decade.
Etiology
- Sporadic – 90%.
- Familial – 10%. May form part of Carney's complex (Carney's, LAMB, NAME syndrome) or non-syndromic familial cardiac myxomas 10,11.
Pathophysiology
- Originate from the endocardium. Composed of embryonic multipotential mesenchymal cells that persist during cardiac septation which can differentiate into angioblasts, fibroblasts, cartilage and myoblasts.
- Macroscopic – Polypoid > villous, papillary often with associated thrombus
- Polypoid – Pedunculated > sessile. Smooth, round mass with low tendancy to fragment.
- Villous - Gelatinous extensions, greater fragmentation and embolic risk.
- Sizes range from 1 – 15 cm, majority 5 – 6 cm with variable growth rate17
Site
- LA (75 -80%) > RA (15-20%) > LV (3-4%) > RV (3-4%), fig. 1, 2a and 2b.
- LA myxomas origins: IAS at fossa ovalis border(75%) > posterior atrial wall > anterior atrial wall > atrial appendage
- Rare sites - Valvular myxomas (MV > TV > AV > PV) 3,13, biatrial myxomas 1, 2, 12 , fig. 3
- Multiple tumours are more commonly seen among familial series.
{kind=link}
Clinical Presentation
- Depends on location, size and mobility. Masquerades as other intracardiac pathology, most commonly mitral valve disease1.
- Embolism 30-40% patients
- Left sided myxomas Cerebral (stroke), retinal arteries (visual loss)
- Right sided myxomas Embolize to the pulmonary vasculature resulting in pulmonary hypertension or lethal pulmonary embolism.
- Risk factors Include a villous surface and tumour vegetation1, 19.
- Intracardiac obstruction LA, RA and ventricular tumours mimic symptoms of mitral stenosis, tricuspid stenosis, and outflow obstruction respectively. Presence of PFO and RA myxoma can cause cyanosis and systemic embolization.
- Valvular regurgitation From tumours impeding atrioventricular valve systolic closure or the to-and-fro movement of the myxoma can traumatize the valve or subchordal structures known as the 'ball wrecking' effect.
- Arrhythmias Atrial or ventricular arrhythmias seen within atrial and ventricular myxomas respectively
- Syncope Results from complete obstruction of MV, TV or arrhythmias
- Sudden cardiac death From MV or TV obstruction, coronary embolization, malignant arrhythmia
- General 40-50% patients experience constitutional symptoms of fatigue, fever, rash, arthralgia, myalgia, weight loss, anemia, raised ESR and CRP, haemolysis, polycythaemia, clubbing. Etiology of symptoms is associated with tumour embolization, complement activation and the secretion of IL625
- Frequency of symptoms Dyspnoea 80% > palpitations 26% > syncope 16% = pedal oedema 16% > chest pain 13%. Asymptomatic in 20%1, 12, 16, 18
- Syndromes - Carney's Complex (Carney's Syndrome, Syndrome Myxoma)
- Sporadic or autosomal dominant inheritance (chromosomes 2,12,17)
- Multiple phenotypic variations expressed but commonly present with intracardiac myxomas, cutaneous disease (lentigines, ephelides, blue naevi), extracardiac myxomas (skin, breast, brain, testis, adrenal and thyroid gland), non-myxomatous tumours (pituitary adenoma, breast fibroadenoma, schwannoma), endocrinopathies (Cushing's syndrome, pituitary and thyroid dysfunction)
- Multiple in 50% patients with atypical locations and higher incidence of recurrence
- Present at a younger age, mean 25 yrs and exhibits no gender bias4
- Previous acronyms include NAME (Naevi, Atrial myxoma, Myxoid neurofibroma and Ephelides) and LAMB syndrome (Cutaneous Lentigines, Atrial myxoma, Mucocutaneous myxoma and Blue naevi) which have been collated under Carney's complex10
Imaging &Investigations
- Exclude other intracardiac masses
- Chest XRay Enlarged LA, tumour calcification, pulmonary edema
- CT/MRI Good delineation of size, extent and solid/cystic tumour content
- Angiography Not used for diagnosis. Tumour depicted by intracavity filling defect. Coronary angiography used to identify associated coronary disease in patients above 40 yrs, branches of the coronary system supplying the tumour, coronary tumour thrombosis and aneurysmal dilatations.
- Echocardiograpy TEE provides better tumour definition, identifies multiple masses, location, extent of tumour attachment and associated thrombus compared to TTE. See below echo details.
Differential Diagnosis
- Exclude other intracardiac masses
- Benign tumours Lipoma, papillary fibroelastoma, fibroma, angioma, rhabdomyoma
- Malignant tumours Angiosarcoma, rhabdosarcoma, synovial sarcoma, others myofibroblastic differentiated sarcomas (fibrosarcoma, osteosarcoma, histiocytoma, leiomyosarcoma), lymphoma, metastases
- Thrombus
- Vegetation
Indicators for Surgical Intervention
- Curative (excisional biopsy)
- Prevent embolic complications
Surgical Options
- Bicaval and aortic cannulation enables access of the RA or LA. Low or high lying RA tumours may necessitate SVC/brachiocephalic and femoral cannulation or deep hypothermic circulatory arrest, fig 5 and 6.
- Surgical excision of tumour and stalk with 5 mm margin of normal tissue is recommended to reduce the risk of recurrence with direct or pericardial/Dacron patch closure of ASD. Avoid tumour fragmentation on excision with good irrigation and suction to reduce the risk of distal embolization.
- Valvular damage will necessitate valve repair/replacement.
{kind=link}
{kind=link}
Complications
- Infected myxoma Rare complication with the formation of vegetations20
- Malignant transformation Controversial. Associated with multiple distant metastasis of recurrent cardiac myxomas7
Survival
- Operative mortality 0 – 3%. Low risk of post-operative arrhythmias or permanent pacemaker.
- Recurrence
- Sporadic myxomas 1 – 3%. Due to incomplete resection or intraoperative displacement of tumour material.
- Familial Myxomas 12 – 22%. Due to multifocal genesis.
- Monitoring IL6 could be used to follow patients for recurrence6,25,26
- Follow-up echocardiography recommended butinterval remains controversial. Closer follow-up required for familial tumours, atypical locations, younger patients, multiple lesions or altered genotype.
Figures &Videos
- Fig. 1a 2D midesophageal 4 chamber demonstrating a smooth polypoid left atrial myxoma.
- Fig. 1b 3D full volume of the MV LAX displaying a large left atrial myxoma prolapsing through the mitral valve.
- Fig. 1c 3D full volume of a left atrial myxoma viewed from the left atrium.
- Fig. 1d 3D full volume of the RV inflow demonstrating a left atrial myxoma attached to the interatrial septum.
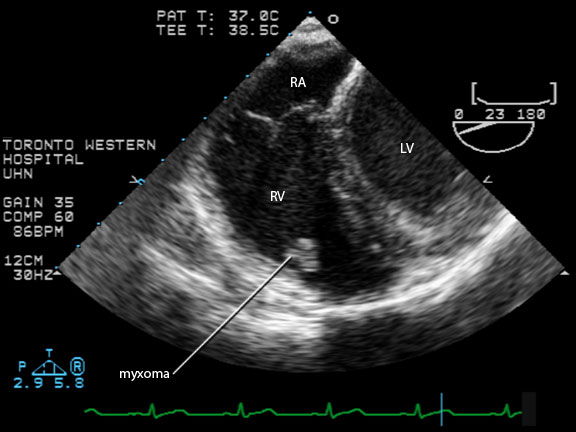
- Fig. 2a 2D midesophageal RV in/outflow view demonstrating a myxoma adherent to the right ventricular free wall in a patient with Carney's complex.
- Fig. 2b 2D midesophageal RV in/outflow view demonstrating a myxoma adherent to the right ventricular free wall in a patient with Carney's complex. RA = Right atrium, RV = Right Ventricle, LV = Left Ventricle.
- Fig. 3 2D midesophageal 4 chamber view displaying a biatrial myxoma.
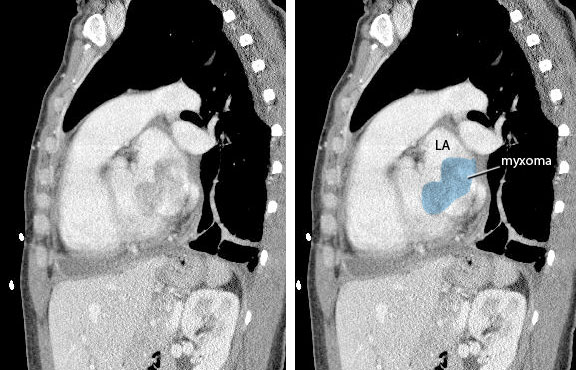
- Fig. 4 Coronal cardiac CT slice demonstrating a left atrial myxoma.
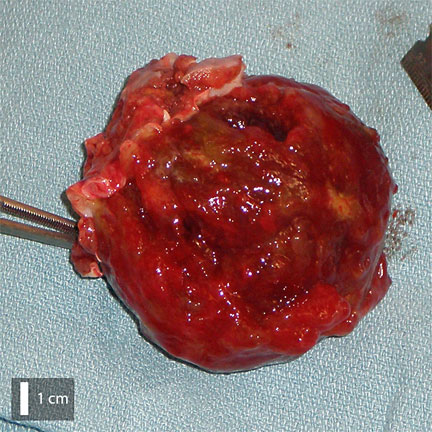
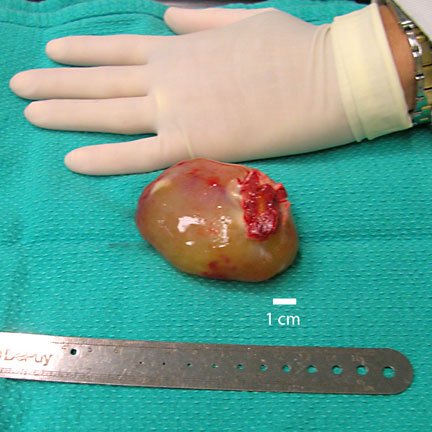
- Fig. 5 Hemorrhagic left atrial myxoma.
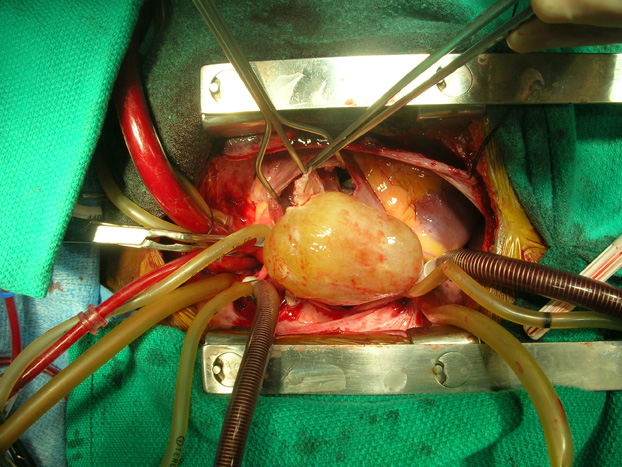
- Fig. 6a Intraoperative view of a large left atrial myxoma accessed through the right atrium whilst on cardiopulmonary bypass
- Fig. 6b Large polypoid left atrial myxoma
- Fig. 7 Left atrial myxoma with finger-like villous surface projections
- Fig. 8 2D midesophageal 4 chamber view of a left atrial myxoma with bright calcific and echolucent necrotic areas
- Fig. 9 Left atrial myxoma prolapsing through the mitral valve causing 'functional' mitral stenosis and incomplete mitral valve closure leading to mitral regurgitation
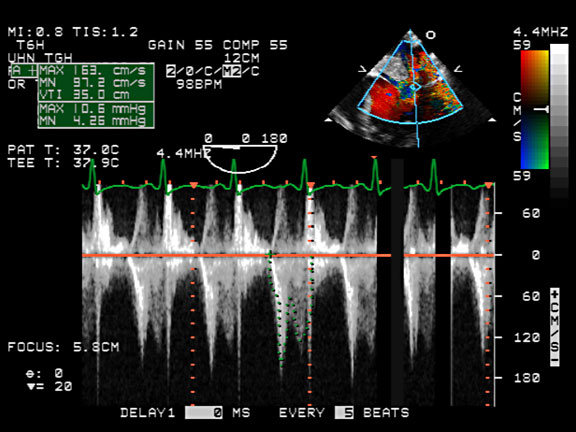
- Fig. 10 Transmitral pulse wave Doppler demonstrating mild mitral stenosis
{kind=link}
{kind=link}
{kind=link}
Echo Features
What to look for in 2D and 3D TEE
- Single or multiple masses
- Location + size + mobility
- Attachment site + length/width stalk
- Smooth or villous surface appearance, fig. 1 and 7
- Calcified echogenic area
- Hemorrhagic (necrotic) echolucent areas, fig. 8
- Prolapse of myxoma through atrioventricular valve. Depends on size and presence of stalk. Tumours which do not prolapse have no stalk or are either too small or too large
- Trauma to valvular + subchordal structures
What to look for in Colour Doppler
- Flow acceleration through stenotic valves
- Valvular regurgitation, fig.9
What to look for in Spectral Doppler
- Severity valvular stenosis peak/mean pressure gradients, PHT, DT, fig. 10
- Severity valvular regurgitation
Differential Diagnosis
Papillary Fibroelastoma
- Benign, small, mobile mass located on atrioventricular or semilunar valves 22,23. Usually on left side of the heart of older patients and typically downstream of valve (LV side in MV PFE, aortic side in AV PFE)
- Associations – thromboembolic complications
Lipoma
- Benign, well encapsulated and homogenous tumours located at any position within the heart and demonstrates no age or gender bias 22,23.
- Subepicardial tumours may compress the heart and cause a pericardial effusion.
- Subendocardial tumours are usually found within the RA and LV and may lead to chamber obstruction.
- Fatty infiltration of IAS spares fossa ovalis producing a dumb-bell shaped septum which is > 1.5 cm thick. Lipomas within IAS and myocardium may cause arrhythmias. IAS lipomas are more prevalent among elderly, women and obese patients.
Fibroma
- Benign intraventricular tumour, well demarcated mass with foci of calcification, 1-10 cm diameter
- Associations – childhood tumour, may lead to ventricular obstruction
Rhabdomyoma
- Benign, well circumscribed, pedunculated ventricular mass. Maybe multiple in number.
- Associations – commonest pediatric tumour, tuberous sclerosis (seizures, developmental delay, multiple solid end organ tumours) and may lead to ventricular obstruction
Angioma
- Benign subendocardial nodules, 2-4 cm diameter, usually within interventricular septum,
- Associations – tumour blush on angiography 14
Angiosarcoma
- Malignant tumour, broad base nodular or lobular mass, commonly located within the RA close to the IVC. Locally invasive with spread to pleura, mediastinum and pericardium with associated effusion.
- Associations – male predominance, peak incidence in 4th decade, commonest sarcoma
Rhabdosarcoma
- Located in any cardiac chamber
- Associations – male predominance, 2nd commonest cardiac sarcoma
Metastases
- Commonest malignant cardiac tumour from distal solid organ and haematological malignancies.
- Frequency in descending order - leukaemia (54%) > melanoma (34%) > bronchogenic > sarcoma > breast > esophageal > ovarian > kidney > colonic 22
Associated Conditions
Infected Myxoma
- Vegetation adherent to myxoma.
Pleural effusions
- Secondary to left sided valvular obstruction/regurgitation.
References
- Reynen K. Cardiac myxomas. NEJM 1995;333:1610-7
- Irani AD et al. Biatrial myxomas: A case report and review of the literature. J Card Surg 2008;23:385-90
- Oliveira RG et al. Mitral valve myxomas: an unusual entity. Eur J Echocard 2008;9:181-3
- Kazakis DJ et al. Transesophageal echocardiography in the evaluation of cardiac myxoma: a case of familial myxoma. Clin Cardiol 1995;18:283-5
- Desousa AL et al. Atrial myxoma: a review of the neurological complications, metastases and recurrences. J Neurol Neurosurg Psych 1978;41:1119-24
- Mendoza et al. Interleukin-6 production and recurrent cardiac myxoma. J Thorac Cardiovasc Surg 2001;121:395-6
- Hou YC et al. Recurrent cardiac myxoma with multiple distant metastasis and malignant change. J Formos Med Assoc 2001;100:63-5
- Keeling IM et al. Cardiac myxomas: 24 years of experience in 49 patients. Eur J Cardiothorac Surg 2002;22:971-7
- Farah MG. Familial cardiac myxoma. A study of relatives of patients with myxoma. Chest 1994;105:65-8
- Casey M et al. Identification of a novel genetic locus for familial cardiac myxomas and Carney complex. Circ 1998;98:2560-6
- Dandolu BR et al. Nonsyndrome familial atrial myxoma in two generations. J Thorac Cardiovasc Surg 1995;110:872-4
- Goswami KC et al. Cardiac myxomas: clinical and echocardiographic profile. Int J Cardiol 1998;63:251-9
- Yuan SM et al. Tricuspid valve myxoma: a case report and a collective review of the literature. J Card Surg 2009;24:69-72
- Shapiro LM. Cardiac tumours: diagnosis and management. Heart 2001;85:218-22
- Hsieh PU et al. Echocardiographic features of primary cardiac sarcoma. Echocardiography 2002;19:215-20
- Burke A et al. Cardiac tumours: an update. Heart 2009;94:117-23
- Karlof E et al. How fast does an atrial myxoma grow? Ann Thorac Surg 2006;82:1510-2
- Aggarwal SK et al. Clinical presentation and investigation findings in cardiac myxomas: new insights from the developing world. Am Heart J 2007;154:1102-7
- Acebo E et al. Clinicopathologic study and DNA analysis of 37 cardiac myxomas. Chest 2003;123:1379-85
- Ten Berg JM et al. Endocarditis on a left atrial myxoma. Eur Heart J 1992;13:1592-3
- Yao F et al. Infective mitral valve myxoma with coronary artery embolization: surgical intervention followed by prolonged survival. J Thorac Cardiovasc Surg 2009;137:749-51
- Walkes JCM et al. Cardiac Neoplasms. Cardiac surgery in the adult, Cohn LH, 3rd edition, McGraw-Hill 2008:1479 -1510
- Sidebotham D et al. Practical perioperative tranoesophageal echocardiography, Butterworth-Heinemann 2003.
- Wilkes D et al. Inherited disposition to cardiac myxoma development. Nature Rvw Cancer 2006;6:157-65
- Seino Y et al. Increased expression of interleukin 6 mRNA in cardiac myxomas. Br Heart J 1993;69:565-7
- Kanda T et al. Interleukin-6 and cardiac myxoma. Am J Cardiol 1994;74:565-6
Abbreviations
| Abbreviation | Term |
|---|---|
| AI /AR | Aortic Insufficiency/ regurgitation |
| AoArch | Aortic arch |
| AS | Aortic stenosis |
| AscAo | Ascending aorta |
| ASD | Atrial septal defect |
| AV | Aortic Valve |
| AVN | Atrioventricular node |
| CBF | Coronary blood flow |
| Ch | Chamber |
| CRP | C reactive protein |
| CW | Continuous wave Doppler |
| DT | Deceleration time |
| ESR | Erythrocyte sedimentation rate |
| IAS | Interatrial septum |
| IL 6 | Interleukin 6 |
| IVC | Inferior vena cava |
| IVS | Interventricular septum |
| L | Left |
| LAX | Long axis view |
| LV | Left ventricle |
| LVOT | Left ventricular outflow tract |
| ME | Midesophageal view |
| mPA | Main pulmonary artery |
| MR | Mitral Regurgitation |
| MV | Mitral valve |
| R | Right |
| RA | Right atrium |
| RCC | Right coronary cusp |
| RV | Right ventricle |
| RVOT | Right ventricular outflow tract |
| RVSP | Right ventricular systolic pressure |
| PA | Pulmonary artery |
| PASP | Pulmonary artery systolic pressure |
| PDA | Patent ductus arteriosus |
| PFE | Papillary fibroelastoma |
| PFO | Patent foramen ovale |
| PHT | Pressure half time |
| PV | Pulmonary valve |
| PW | Pulse wave Doppler |
| SAX | Short axis view |
| SVC | Superior vena cava |
| TG | Transgastric view |
| TEE | Transesophageal echocardiography |
| TTE | Transthoracic echocardiography |
| UE | Upper esophageal view |
| VTI | Velocity time integral |